
Table of Contents
Meaningful Use Measure Recording
Medication Allergy List - Stage 1
CPOE - Medication Orders Stage 1
CPOE – Medication Orders Alternative Stage 1 / Stage 2
CPOE – Laboratory Orders Stage 2
CPOE – Radiology Orders Stage 2
Demographics – Stage 1 & Stage 2
Medication Reconciliation - Stages 1 & 2
Family Health History - Stage 2
Meaningful Use Measure Reporting
Clinical Quality Measure Recording
Clinical Quality Measure Reporting
Client
Record Changes

A. Some of the buttons previously located at the bottom of the Client Record are now tabs across the top of the Client Record
1. Vital Signs
2. Smoking Status
3. Activity Rates
4. Labs
5. Immunizations
B. Several new tabs were added across the top of the Client Record
1. Family Health History
2. Record Requests
3. Clinical Summary
4. Cognitive Status
5. Care Plan
C. The following buttons remain at the bottom of the Client Record
1. Update
2. Update and Send Invite to Patient Portal
3. Address History
4. Emergency Contacts Report
5. Scan Driver’s License
6. Help
Meaningful Use Measure Recording
Related Links:
1. CMS site on MU attestation: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Meaningful_Use.html
2. Stage 1 measures: https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/EP-MU-TOC.pdf
3. Stage 2 measures: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_TableContents_EPs.pdf
Problem
List – Stage 1
|
|
|
|
|
|
|
|
|
|
|
|
|
Objective:
Maintain an up-to-date problem list of current and
active diagnoses. Measure: More than 80 percent of all unique patients seen
by the EP have at least one entry or an indication that no problems are known
for the patient recorded as structured data. Exclusion: No exclusion. Numerator: Number of patients in the denominator
who have at least one entry (or an indication that no problems are known)
recorded as structured data in their problem list |
|
||||||||||
|
Denominator: Number of unique patients seen by the
EP during the EHR reporting period |
|||||||||||
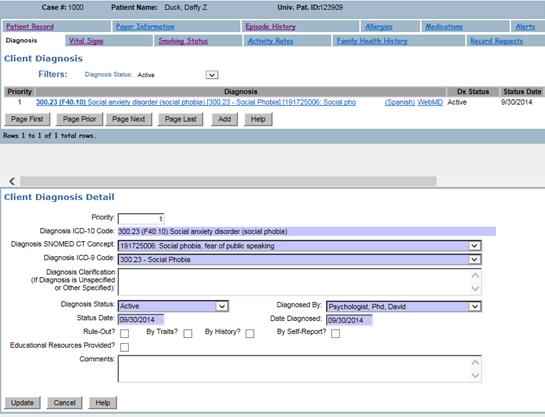
A. Problem list information must be recorded on the Diagnosis tab on the Client Record in Epitomax
1. A SNOMED Concept must be selected for each Diagnosis for MU.
2. You can choose to require a SNOMED Concept for each diagnosis entered by setting the DIAGNOSIS_REQUIRE_SNOMEDCT company constant to TRUE in code table maintenance.
B. The client must be seen by the EP within the reporting period to be credited for MU.
Medication List - Stage 1Objective: Maintain active medication list. Measure: More than 80 percent of all unique patients seen by the EP have at least one entry (or an indication that the patient is not currently prescribed any medication) recorded as structured data. Exclusion: No exclusion. Numerator: Number of patients in the denominator who have at least one entry (or an indication that no medications are prescribed) recorded as structured data in their medication list Denominator: Number of unique patients seen by the EP during the EHR reporting period |
A.
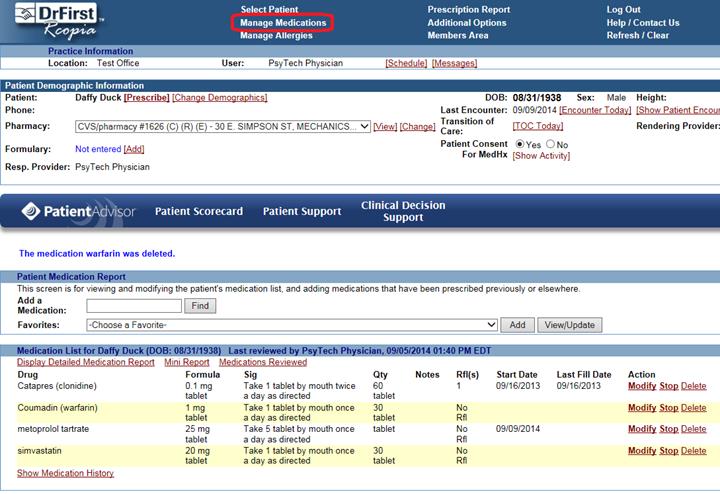
The Medication List is recorded in DrFirst.
B. The client must be seen by the EP within the reporting period to be credited for MU.
Medication Allergy List - Stage 1Objective: Maintain active medication allergy list. Measure: More than 80 percent of all unique patients seen by the EP have at least one entry (or an indication that the patient has no known medication allergies) recorded as structured data. Exclusion: No exclusion. Numerator: Number of unique patients in the denominator who have at least one entry (or an indication of no known medication allergies) recorded as structured data in their medication allergy list Denominator: Number of unique patients seen by the EP during the EHR reporting period |
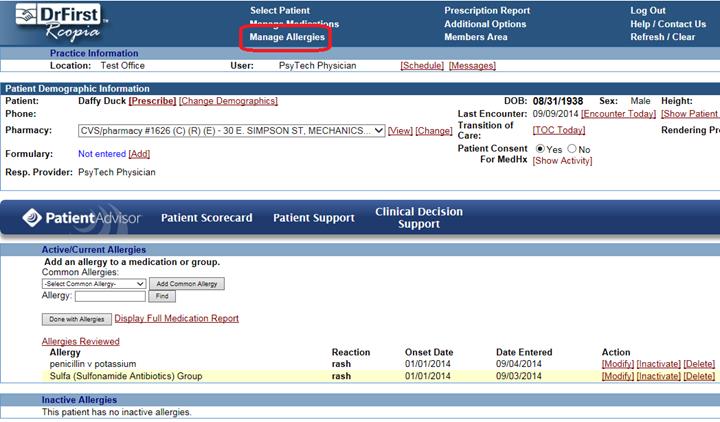
A. The Medication Allergy List is recorded in DrFirst.
B. The client must be seen by the EP within the reporting period to be credited for MU.
CPOE
- Medication Orders Stage 1
|
|
|
|
|
|
|
|
|
|
|
|
|
Objective:
Use computerized provider order entry (CPOE) for
medication orders directly entered by any licensed healthcare professional
who can enter orders into the medical record per state, local and
professional guidelines. Measure: More than 30 percent of all unique patients with at least one medication in their medication list seen by the EP have at least one medication order entered using CPOE. Exclusion: Any EP who writes fewer than 100 prescriptions
during the EHR reporting period. Numerator: Number of patients in the
denominator that have at least one medication order entered using CPOE |
|
||||||||||
|
Denominator: Number of unique patients with
at least one medication in their medication list seen by the EP during the
EHR reporting period |
|||||||||||
A.
Medication Orders are recorded in DrFirst.
1.
Any medication that the EP ePrescribes in
DrFirst is an Order entered using CPOE, and will count towards this measure.
B. The client must be seen by the EP within the reporting period to be credited for MU.
CPOE
– Medication Orders Alternative Stage 1 / Stage 2
|
|
|
|
|
|
|
|
|
|
|
|
|
Objective:
Use computerized provider order entry (CPOE) for medication
orders directly entered by any licensed healthcare
professional who can enter orders into the medical record per state, local
and professional guidelines. Measure: More than 30 percent during stage 1 and more than 60 percent during stage 2 of medication orders created by the EP during the EHR reporting period are recorded using CPOE. Exclusion:
Any EP who writes fewer than 100 medication orders
during the EHR reporting period. Numerator: Number of medication orders in
the denominator recorded using CPOE |
|
||||||||||
|
Denominator: Number of medication orders
created by an EP during the EHR reporting period |
|||||||||||
A.
Medication Orders are recorded in DrFirst.
1.
Any medication that the EP ePrescribes in
DrFirst is an Order entered using CPOE, and will count towards this measure.
B. The client must be seen by the EP within the reporting period to be credited for MU.
CPOE
– Laboratory Orders Stage 2
|
|
|
|
|
|
|
|
|
|
|
|
|
Objective:
Use computerized provider order entry (CPOE) for laboratory
orders directly entered by any licensed healthcare
professional who can enter orders into the medical record per state, local
and professional guidelines. Measure: More than 30 percent of laboratory orders created by the EP during the EHR reporting period are recorded using CPOE. Exclusion:
Any EP who writes fewer than 100 laboratory orders
during the EHR reporting period. Numerator: Number of laboratory orders in
the denominator recorded using CPOE |
|
||||||||||
|
Denominator: Number of laboratory orders
created by an EP during the EHR reporting period |
|||||||||||
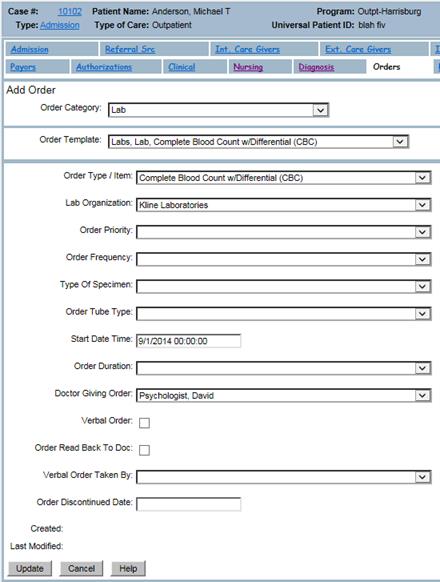
A. Lab Orders must be recorded in Epitomax
1. Lab Orders are entered on the Orders tab of the Admission with an Order Category of “Lab”
2. Set the staff to the EP
3. The Start Date is used when looking for a particular Reporting Period
B. All lab orders are CPOE.
CPOE
– Radiology Orders Stage 2
|
|
|
|
|
|
|
|
|
|
|
|
|
Objective:
Use computerized provider order entry (CPOE) for
radiology orders directly entered by any licensed healthcare professional who
can enter orders into the medical record per state, local and professional
guidelines. Measure: More than 30 percent of radiology orders created by the EP during the EHR reporting period are recorded using CPOE. Exclusion:
Any EP who writes fewer than 100 radiology orders
during the EHR reporting period. Numerator: Number of radiology orders in
the denominator recorded using CPOE |
|
||||||||||
|
Denominator: Number of radiology orders
created by an EP during the EHR reporting period |
|||||||||||
A. Radiology Orders must be recorded in Epitomax
1. Radiology Orders are entered on the Orders tab of the Admission as an Order Category of “Radiology”
2. Set the staff to the EP
3. The Start Date is used when looking for a particular Reporting Period
B. All radiology orders are CPOE.
ePrescribing (eRx)Stage 1 Objective: Generate and transmit permissible prescriptions electronically (eRx). Measure: More than 40 percent of all permissible prescriptions written by the EP are transmitted electronically using certified EHR technology. Exclusion: 1. Any EP who writes fewer than 100 prescriptions during the EHR reporting period. 2. Any EP who does not have a pharmacy within their organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the EP's practice location at the start of his/her EHR reporting period. Numerator: Number of prescriptions in the denominator transmitted electronically Denominator: Number of prescriptions written for drugs requiring a prescription in order to be dispensed, other than controlled substances, during the EHR reporting period Stage 2 Objective: Generate and transmit permissible prescriptions electronically (eRx). Measure: More than 50 percent of all permissible prescriptions, or all prescriptions, written by the EP are queried for a drug formulary and transmitted electronically using CEHRT. Exclusion: Any EP who: 1. Writes fewer than 100 permissible prescriptions during the EHR reporting period. 2. Does not have a pharmacy within their organization and there are no pharmacies that accept electronic prescriptions within 10 miles of the EP's practice location at the start of his/her EHR reporting period. Numerator: Number of prescriptions in the denominator generated, queried for a drug formulary, and transmitted electronically Denominator: Number of prescriptions written for drugs
requiring a prescription in order to be dispensed, during the EHR reporting
period |
A. ePrescribing is done in DrFirst.
Demographics
– Stage 1 & Stage 2
|
|
|
|
|
Stage 1: Epitomax Name: Patient Demographics Objective: Record
all of the following demographics: (A) Preferred language (B) Gender (C) Race (D) Ethnicity (E) Date of birth Measure:
More than 50 percent of all unique patients seen by the EP have demographics
recorded as structured data. Exclusion:
No exclusion. Stage 2: Epitomax Name: Record Demographics Objective:
Record the following demographics: preferred language, sex, race, ethnicity,
date of birth. Measure:
More than 80 percent of all unique patients seen by the EP have demographics
recorded as structured data. Exclusion:
No exclusion. Numerator: Number of patients in the denominator who
have all the elements of demographics (or a specific exclusion if the patient
declined to provide one or more elements or if recording an element is
contrary to state law) recorded as structured data |
|||
|
Denominator: Number of unique patients seen by the EP
during the EHR reporting period |
|||
A. Demographic information must be recorded on the Client Record in Epitomax
1. Date of Birth.
2. Sex.
3. Language.
a. Declined to Specify is a valid option
4. Ethnicity.
a. Declined to Specify is a valid option
5. Race:
a. Declined to Specify is a valid option
b. Up to 2 races can be specified
B. The Demographic Information fields should be set as Required in Administration>Validation Rules Maintenance.
C. The client must be seen by the EP within the reporting period to be credited for MU.
Vital
Signs
Stage
1: Objective:
Record and chart changes in the following vital
signs: (A) Height (B) Weight (C) Blood pressure (D) Calculate and display body mass index (BMI) (E) Plot and display growth charts for children
2-20 years, including BMI Measure: For more than 50 percent of all unique patients
age 2 and over seen by the EP, height, weight, and blood pressure are
recorded as structured data. New
Measure (Optional 2013; Required 2014 and beyond): For more than 50 percent of all unique patients
seen by the EP during the EHR reporting period have blood pressure (for
patients age 3 and over only) and height and weight (for all ages) recorded
as structured data. Stage
2: Objective: Record and chart changes in the following vital
signs: height/length and weight (no age limit); blood pressure (ages 3 and
over); calculate and display body mass index (BMI); and plot and display
growth charts for patients 0-20 years, including BMI. Measure: More than 80 percent of all unique patients seen
by the EP have blood pressure (for patients age 3 and over only) and/or
height and weight (for all ages) recorded as structured data. Stage
1 (2013 Only) Epitomax
Name: Vital Signs (2013 Only) |
|
||||
|
Numerator: Number of patients in the denominator who
have entries of height/length, weight, and blood pressure recorded as
structured data |
|||||
|
Denominator:
Number of unique patients 2 years of age or
older seen by the EP during the EHR reporting period Exclusion: Any
EP who either sees no patients 2 years or older, or who believes that all
three vital signs of height, weight, and blood pressure of their patients
have no relevance to their scope of practice. |
|
||||
|
Alternate
Stage 1 (2013 Only)/Stage 1 & Stage 2 (2014 Onward) - All Within Scope Epitomax
Name: Vital Signs (2013 Optional, 2014 Onward) - All
Stats Within Scope |
|
||||
|
Numerator: - Patients 3 years of age or older in the
denominator for whom height/length, weight, and blood pressure are recorded; AND - Patients younger than 3
years of age in the denominator for whom height/length and weight are
recorded |
|||||
|
Denominator: Number of unique patients seen by the EP
during the EHR reporting period Exclusion: Any
EP who believes that all three vital signs of height, weight, and blood
pressure have no relevance to their scope of practice is excluded from
recording them; |
|
||||
|
Stage
1 & Stage 2 (BP Out of Scope) Epitomax
Name: Vital Signs (2013 Optional, 2014 Onward) - Height
and Weight Only, Blood Pressure Out of Scope |
|
|
|
|
|
|
Numerator:
Number of patients in the denominator who
have entries of height/length and weight recorded as structured data |
|
||||
|
Denominator: Number of unique patients seen by the EP
during the EHR reporting period Exclusion: Any
EP who 1.
Believes that all three vital signs of height, weight, and blood pressure
have no relevance to their scope of practice is excluded from recording them;
2.
Believes that blood pressure is relevant to their scope of practice, but
height and weight are not, is excluded from recording height and weight. |
|
||||
|
Stage
1 & Stage 2 (Ht/Wt Out of Scope) Epitomax
Name: Vital Signs (2013 Optional, 2014 Onward) - Blood
Pressure Only, Height and Weight Out of Scope |
|
|
|
|
|
|
Numerator: Number of patients in the denominator who
have an entry of blood pressure as structured data |
|
||||
|
Denominator: Number of unique patients 3 years of age or
older seen by the EP during the EHR reporting period Exclusion: Any
EP who 1.
Sees no patients 3 years or older is excluded from recording blood pressure; 2.
Believes that all three vital signs of height, weight, and blood pressure
have no relevance to their scope of practice is excluded from recording them;
3.
Believes that height and weight are relevant to their scope of practice, but
blood pressure is not, is excluded from recording blood pressure; |
|
||||
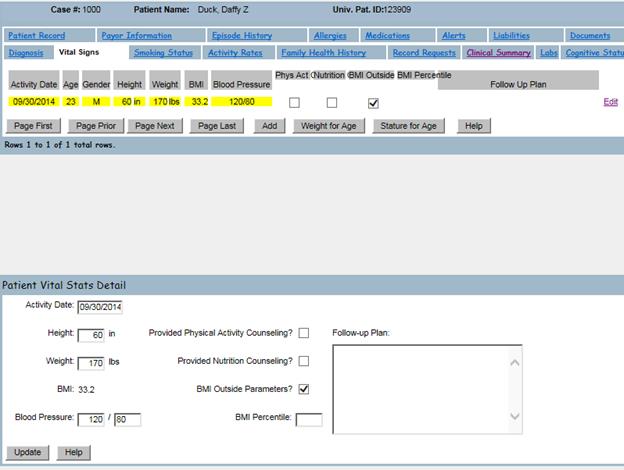
A. Vital Signs can be recorded on the Vital Signs tab of the Client Record in Epitomax
1. Click Add to record the applicable Vital Signs, then click Update
B. Blood Pressure might be out of scope depending on your practice.
C. Height/Weight might be out of scope depending on your practice.
D. The client must be seen by the EP within the reporting period to be credited for MU.
Smoking Status - Stages 1 & 2Objective: Record smoking status for patients 13 years old or older. Measure: More than 50 percent of all unique patients 13 years old or older seen by the EP have smoking status recorded as structured data. Exclusion: Any EP who sees no patients 13 years or older. Numerator: Number of patients in the denominator with smoking status recorded as structured data Denominator: Number of unique patients age 13 or older seen by the EP during the EHR reporting period |
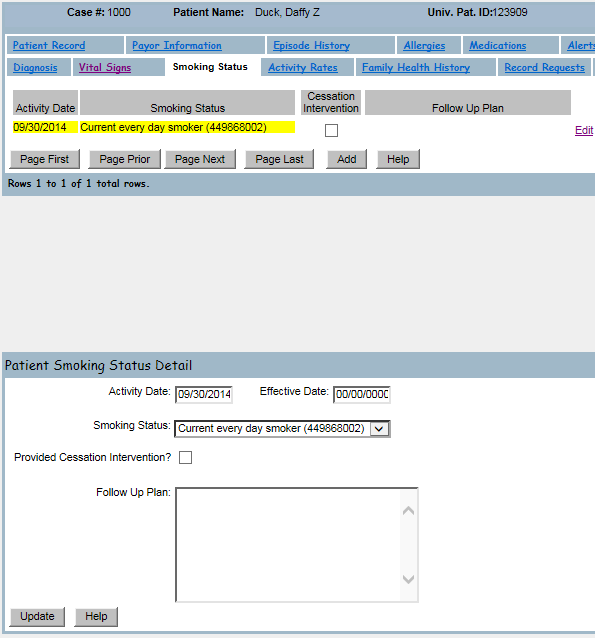
A. Smoking Status is recorded on the Smoking Status tab on the Client Record in Epitomax.
B. The client must be seen by the EP within the reporting period to be credited for MU.
Patient RemindersStage 1 Epitomax Name: Patient
Reminders Objective: Send reminders to patients per patient preference for preventive/follow-up care. Measure: More than 20 percent of all patients 65 years or older or 5 years old or younger were sent an appropriate reminder during the EHR reporting period. Exclusion: An EP who has no patients 65 years old or older or 5 years old or younger with records maintained using certified EHR technology. Numerator: Number of patients in the denominator who were sent the appropriate reminder during the reporting period Denominator: Number of unique patients 65 years of age or older or 5 years of age or younger Stage 2 Epitomax Name: Patient Reminders for F/U Care Objective: Use clinically relevant information to identify patients who should receive reminders for preventive/follow-up care and send these patients the reminders, per patient preference. Measure: More than 10 percent of all unique patients who have had 2 or more office visits with the EP within the 24 months before the beginning of the EHR reporting period were sent a reminder, per patient preference when available. Exclusion: Any EP who has had no office visits in the 24 months before the EHR reporting period. Numerator: Number of patients in the denominator who were sent a reminder per patient preference, when available, during the EHR reporting period Denominator: Number of unique patients who have had two or more office visits with the EP in the 24 months prior to the beginning of the EHR reporting period |
A. Reminders for preventative / follow-up care are entered on the Scheduling / Reminder History screen. This menu item is only available after opening a client’s record.
a. Only preventative / follow-up care reminders count toward the measure. Appointment reminders do not count.
b. For the stage 2 measure, the reminder must be sent using the client’s preferred contact method.
B. For stage 1, the EP must be an internal care giver on the client’s admission.
C. For stage 2, the client must have 2 visits with the EP in the 24 months prior to the start of the reporting period.

View, Download, TransmitMeasure A (Stages 1 &
2) Epitomax Name – Stage 1: Timely Electronic Access Epitomax Name – Stage 2: Patient Electronic Access, Measure 1 Objective: Provide patients with timely electronic access to their health information (including lab results, problem list, medication lists, and allergies) within 4 business days of the information being available to the EP. Measure – Stage 1: At least 10 percent of all unique patients seen by the EP are provided timely (available to the patient within four business days of being updated in the certified EHR technology) electronic access to their health information subject to the EP’s discretion to withhold certain information. Measure – Stage 2: More than 50 percent of all unique patients seen by the EP during the EHR reporting period are provided timely (available to the patient within 4 business days after the information is available to the EP) online access to their health information, with the ability to view, download, and transmit to a third party. Exclusion – Stage 1: Any EP that neither orders nor creates lab tests or information that would be contained in the problem list, medication list, medication allergy list (or other information as listed at 45 CFR 170.304(g)) during the EHR reporting period. Exclusion – Stage 2: Any EP who: (1) Neither orders nor creates any of the information listed for inclusion as part of both measures, except for "Patient name" and "Provider's name and office contact information,” may exclude both measures. (2) Conducts 50 percent or more of his or her patient encounters in a county that does not have 50 percent or more of its housing units with 3Mbps broadband availability according to the latest information available from the FCC on the first day of the EHR reporting period may exclude only the second measure. Numerator: Number of patients in the denominator who have timely (within 4 business days after the information is available to the EP) online access to their health information Denominator: Number of unique patients seen by the EP during the EHR reporting period Measure B (Stage 2) Epitomax Name: Patient Electronic Access, Measure 2 Objective: Provide patients the ability to view online, download and transmit their health information within four business days of the information being available to the EP. Measure: More than 5 percent of all unique patients seen by the EP during the EHR reporting period (or their authorized representatives) view, download, or transmit to a third party their health information Exclusion: Any EP who: (1) Neither orders nor creates any of the information listed for inclusion as part of both measures, except for "Patient name" and "Provider's name and office contact information,” may exclude both measures. (2) Conducts 50 percent or more of his or her patient encounters in a county that does not have 50 percent or more of its housing units with 3Mbps broadband availability according to the latest information available from the FCC on the first day of the EHR reporting period may exclude only the second measure. Numerator: Number of unique patients (or their authorized representatives) in the denominator who have viewed online, downloaded, or transmitted to a third party the patient's health information Denominator: Number of unique patients seen by the EP during the EHR reporting period |
A. Stage 1 and Stage 2 Measure A:
a. Staff must generate a Clinical Summary for the office visit from the Clinical Summary tab of the Client Record within 4 business days of the activity.
b. Clients must have a Patient Portal account that was created prior to the activity with the EP, or within 4 business days of the activity.
B. Stage 2 Measure B:
a. Staff must generate a Clinical Summary for the office visit from the Clinical Summary tab of the Client Record.
b. Clients must have a Patient Portal account, and must view, download, or transmit to a 3rd party their Clinical Summary.
Clinical SummaryStage 1 Epitomax Name: Provide
Clinical Summaries for each Office Visit Objective: Provide clinical summaries for patients for each office visit. Measure: Clinical summaries provided to patients for more than 50 percent of all office visits within 3 business days. Exclusion: Any EP who has no office visits during the EHR reporting period. Numerator: Number of office visits in the denominator for which the patient is provided a clinical summary within three business days Denominator: Number of office visits conducted by the EP during the EHR reporting period Stage 2 Epitomax Name: Clinical
Summary (Office Visit) Objective: Provide clinical summaries for patients for each office visit. Measure: Clinical summaries provided to patients or patient-authorized representatives within one business day for more than 50 percent of office visits. Exclusion: Any EP who has no office visits during the EHR reporting period. Numerator: Number of office visits in the denominator where the patient or a patient-authorized representative is provided a clinical summary of their visit within one business day Denominator: Number of office visits conducted by the EP during the EHR reporting period |
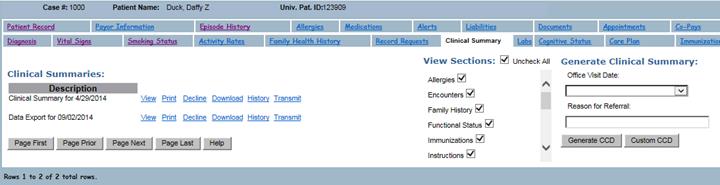
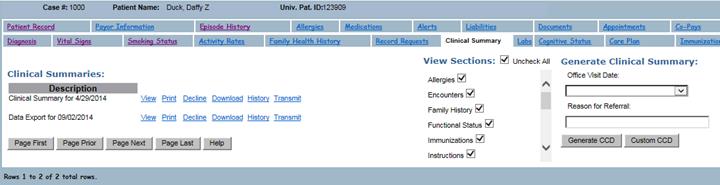
A. Clinical Summaries are generated from the Clinical Summary tab on the Client Record. Select the office visit from the drop down, and click the “Generate CCD” button.
B. Either the client must have a Patient Portal account, or you must provide the summary to the client using the “Print”, “Decline”, or “Download” links for the clinical summary.
C. If a client declines a Clinical Summary, indicate that by clicking the “Decline” link for the Clinical Summary. Otherwise it will not count towards the measure.
D. Clinical Summaries generated using the “Custom CCD” button are not counted because information may have been excluded from the summary.
Patient EducationStage 1 Objective: Use certified EHR technology to identify patient-specific education resources and provide those resources to the patient if appropriate. Measure: More the 10 percent of all unique patients seen by the EP are provided patient-specific education resources. Exclusion: No exclusion. Numerator: Number of patients in the denominator who are provided patient-specific education resources Denominator: Number of unique patients seen by the EP during the EHR reporting period Stage 2 Objective: Use clinically relevant information from Certified EHR Technology to identify patient-specific education resources and provide those resources to the patient. Measure: Patient-specific education resources identified by Certified EHR Technology are provided to patients for more than 10 percent of all unique patients with office visits seen by the EP during the EHR reporting period. Exclusion: Any EP who has no office visits during the EHR reporting period. Numerator: Number of patients in the denominator who were provided patient-specific education resources identified by the EHR technology Denominator: Number of unique patients with office visits seen by the EP during the EHR reporting period |
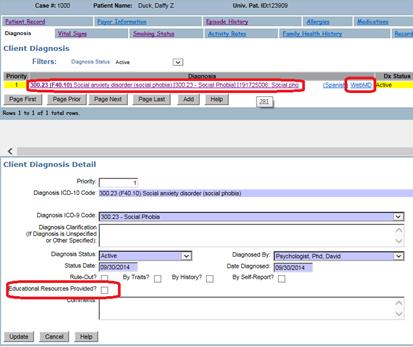
A. Educational resources for Problems are provided from the Diagnosis tab on the Client Record.
a. Click the Diagnosis link (MedlinePlus) or the WebMD link to retrieve educational resources.
b. Also indicate resources were provided for that diagnosis by clicking the edit link, checking the “Educational Resources Provided?” box, and updating.
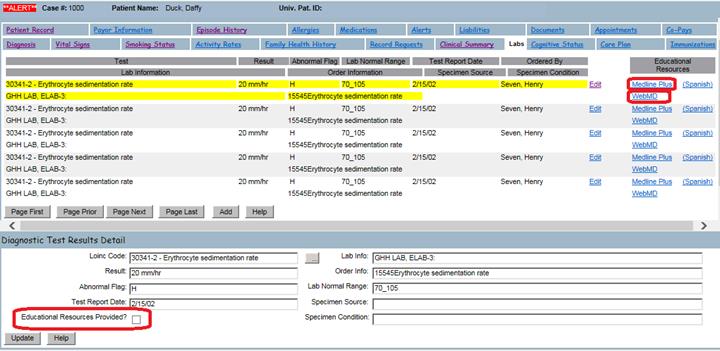
B. Educational resources for Labs are provided from the Labs tab on the Client Record.
a. Click the Medline Plus or WebMD link to retrieve educational resources.
b. Also indicate resources were provided for that lab by clicking the edit link, checking the “Educational Resources Provided?” box, and updating.
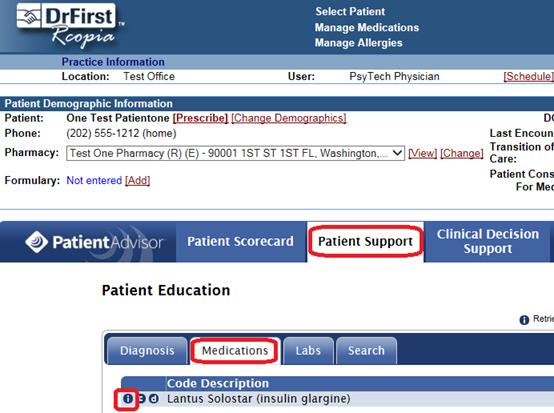
C. Educational resources for Medications are provided from the PatientAdvisor Patient Support tab in DrFirst.
D. The client must be seen by the EP within the reporting period to count towards the measure.
Medication Reconciliation - Stages 1 & 2Objective: The EP who receives a patient from another setting of care or provider of care or believes an encounter is relevant should perform medication reconciliation. Measure: The EP who performs medication reconciliation for more than 50 percent of transitions of care in which the patient is transitioned into the care of the EP. Exclusion: Any EP who was not the recipient of any transitions of care during the EHR reporting period. Numerator: The number of transitions of care in the denominator where medication reconciliation was performed Denominator: Number of transitions of care (defined as first encounters with a new patient and encounters with existing patients where a summary of care record of any type is provided to the receiving provider) during the EHR reporting period for which the EP was the receiving party of the transition |
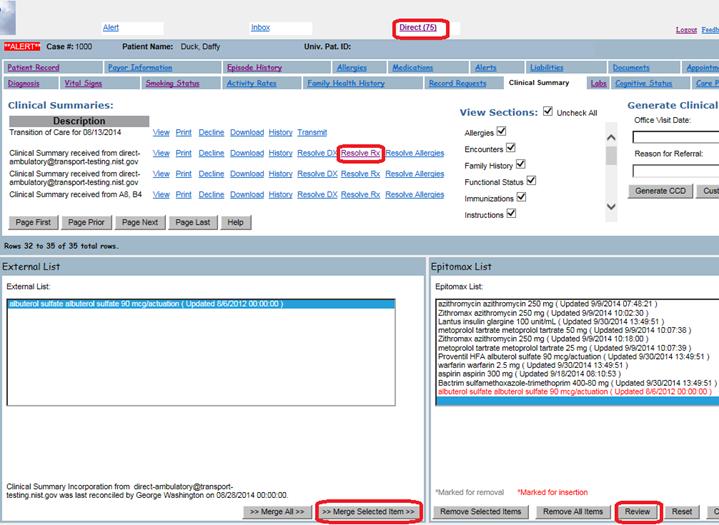
A. An electronic Medication Reconciliation is performed on the Clinical Summary tab of the Client Record.
a. A Transition of Care CCD must be received via the DirectProject from another provider.
b. Open the EP’s Direct messaging inbox from the top of the screen in Epitomax.
c. Open the message containing the CCD, select the attachment, and click the “Copy to Client Record” link.
d. Once on the Clinical Summary tab, click the “Incorporate” link for the newly received Transition of Care.
e. Click the “Resolve Rx” link, and set RxNorm codes for each medication.
f. On the following screen, reconcile the incoming medication list from the Transition of Care with the existing medication list in Epitomax.
g. Click the “Review” button.
h. Click “Update”.
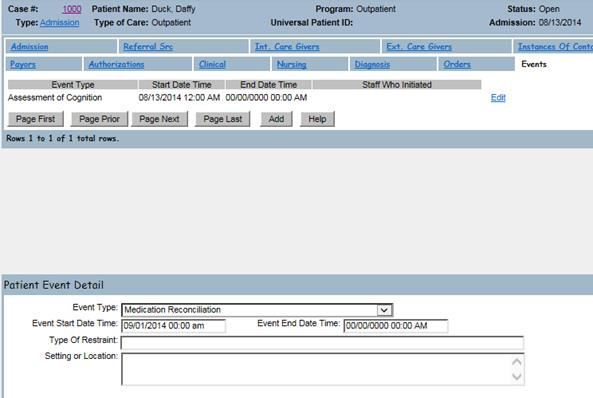
B. A manual Medication Reconciliation is done by hand, and indicated on the Events tab of the admission.
a. Add an event whose type is “Medication Reconciliation”.
b. Set the event start date to the date the reconciliation was performed.
C. The EP must be an internal care giver for the client.
D. The client’s admission must have the Referral by Physician box checked on the Referral Source tab.
E. The client must have an activity with the EP.
Summary of CareStage 1: Epitomax Name: Summary
Care Record (Referral) Objective: The EP who transitions their patient to another setting of care or provider of care or refers their patient to another provider of care should provide summary care record for each transition of care or referral. Measure: The EP who transitions or refers their patient to another setting of care or provider of care provides a summary of care record for more than 50 percent of transitions of care and referrals. Exclusion: An EP who neither transfers a patient to another setting nor refers a patient to another provider during the EHR reporting period. Stage 2: Objective: The EP who transitions their patient to another setting of care or provider of care or refers their patient to another provider of care should provide summary care record for each transition of care or referral. Measures: EPs must satisfy both of the following measures in order to meet the objective: Measure 1: The EP who transitions or refers their patient to another setting of care or provider of care provides a summary of care record for more than 50 percent of transitions of care and referrals. Measure 1 - Epitomax Name: Summary of Care for Transitions of Care, Measure 1 Measure 1 - Numerator: Number of transitions of care and referrals in the denominator where a summary of care record was provided Measure 1 - Denominator: Number of transitions of care and referrals during the EHR reporting period for which the EP was the transferring or referring provider Measure 2: The EP who transitions or refers their patient to another setting of care or provider of care provides a summary of care record for more than 10 percent of such transitions and referrals either (a) electronically transmitted using CEHRT to a recipient or (b) where the recipient receives the summary of care record via exchange facilitated by an organization that is a NwHIN Exchange participant or in a manner that is consistent with the governance mechanism ONC establishes for the NwHIN. Measure 2 - Epitomax Name: Summary of Care for Transitions of Care, Measure 2 Measure 2 - Numerator: - Number of transitions of care and referrals in the denominator where a summary of care record was electronically transmitted using EHR technology to a recipient - Number of transitions of care and referrals in the denominator where the recipient receives the summary of care record via exchange facilitated by an organization that is a NwHIN Exchange participant - Number of transitions of care and referrals in the denominator where the recipient receives the summary of care record in a manner that is consistent with the governance mechanism ONC establishes for the nationwide health information network Measure 2 - Denominator: Number of transitions of care and referrals during the EHR reporting period for which the EP was the transferring or referring provider Measure 3: An EP must satisfy one of the following criteria: Conducts one or more successful electronic exchanges of a summary of care document, as part of which is counted in "measure 2" (for EPs the measure at §495.6(j)(14)(ii)(B) with a recipient who has EHR technology that was developed designed by a different EHR technology developer than the sender's EHR technology certified to 45 CFR 170.314(b)(2). Conducts one or more successful tests with the CMS designated test EHR during the EHR reporting period. Exclusion: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times during the EHR reporting period is excluded from all three measures. |
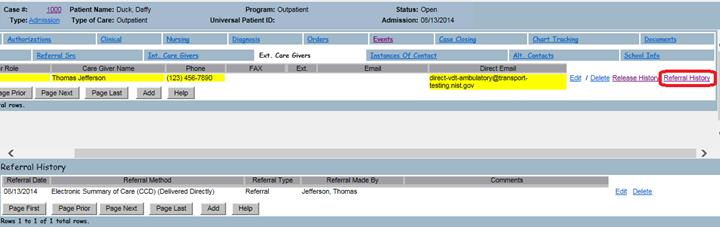
A. A Transition of Care is indicated in Epitomax by adding a Referral made by the EP on the External Care Givers tab of the client’s admission.
B. The EP must be an internal care giver on the client’s admission.
C. Generate a Transition of Care CCD on the Clinical Summary tab. Do not select an Office Visit date, and click the “Generate CCD” button.
D. To Electronically Transmit a Transition of Care CCD:
a. Add the provider care is being transitioned to as an External Care Giver on the client’s admission. Set the provider’s DirectProject email address.
b. Add a referral made by the EP.
c. Add a release of information for the external care giver.
d. Go to the Clinical Summary tab of the Client Record, and click the Transmit link for the Transition of Care CCD. (Note, the staff logged in when transmitting must have a DirectProject email address entered in Staff Maintenance.)
E. To Manually Transmit a Transition of Care CCD:
a. Add the provider care is being transitioned to as an External Care Giver on the client’s admission.
b. Add a referral made by the EP.
c. Add a release of information for the external care giver.
d. Go to the Clinical Summary tab of the Client Record, and print or download the Transition of Care and provide it to the provider.
F. Clinical Summaries generated using the “Custom CCD” button are not counted because information may have been excluded from the summary.


Secure Messaging - Stage 2Objective: Use secure electronic messaging to communicate with patients on relevant health information. Measure: A secure message was sent using the electronic messaging function of CEHRT by more than 5 percent of unique patients (or their authorized representatives) seen by the ep during the EHR reporting period. Exclusion: Any EP who has no office visits during the EHR reporting period, or any EP who conducts 50 percent or more of his or her patient encounters in a county that does not have 50 percent or more of its housing units with 3Mbps broadband availability according to the latest information available from the FCC on the first day of the EHR reporting period. Numerator: Number of patients or patient-authorized representatives in the denominator who send a secure electronic message to the EP that is received using the electronic messaging function of the EHR technology during the EHR reporting period Denominator: Number of unique patients seen by the EP during the EHR reporting period |
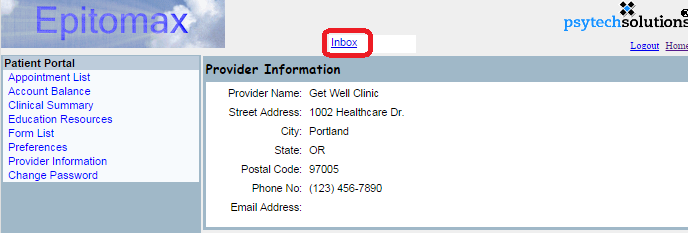
A. The Client must have a Patient Portal account to send the EP a secure message.
B. The EP must be an internal care giver for the client.
C. Client sends the EP a secure message using the “Inbox” link at the top of the Patient Portal.
a. Client can either compose a new message, or reply to an existing one.

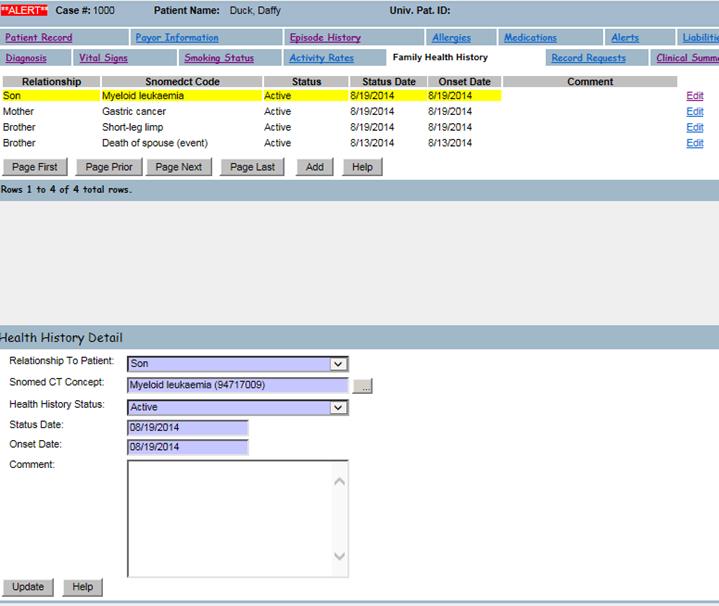
Family Health History - Stage 2Objective: Record patient family health history as structured data. Measure: More than 20 percent of all unique patients seen by the EP during the EHR reporting period have a structured data entry for one or more first-degree relatives. Exclusion: Any EP who has no office visits during the EHR reporting period. Numerator: Number of patients in the denominator with a structured data entry for one or more first-degree relatives (parents, siblings, and offspring) Denominator: Number of unique patients seen by the EP during the EHR reporting period |
A. Family Health History is recorded on the Family Health History tab on the client record.
B. Health history is recorded using SNOMED CT Concepts.
Electronic Notes - Stage 2Objective: Record electronic notes in patient records. Measure: Enter at least one electronic progress note created, edited and signed by an EP for more than 30 percent of unique patients with at least one office visit during the EHR reporting period. The text of the electronic note must be text searchable and may contain drawings and other content Exclusion: Any EP who has no office visits during the EHR reporting period. Numerator: Number of unique patients in the denominator who have at least one electronic progress note from an eligible professional recorded as text-searchable data Denominator: Number of unique patients with at least one office visit for EPs during the EHR reporting period |
A. Electronic Notes in Epitomax are forms whose type is Progress Note.
B. The EP must create, modify, and sign the note. The note will count towards the measure at any point in the create, modify, sign workflow.
C. The Progress Note must be associated with an activity with the EP during the reporting period.
Meaningful
Use Measure Reporting
A. Code Tables
1. Added new Meaningful Use Measure Reporting Period code table.
a. Additional reporting periods can be entered in this table, particularly if you are reporting for a 3 month period
b. Reporting periods can be deactivated in this table
c. This same code is used for both Clinical Quality Measure and Meaningful Use Measure Reporting Periods
B. Meaningful Use Measure Calculation for each Eligible Provider (EP)
1. Administration Reports>Meaningful Use Measure Calculation
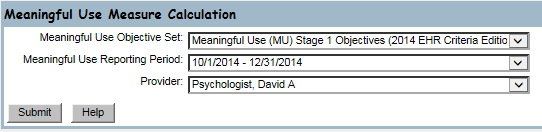
a. Select a Meaningful Use Objective Set
b. Select a Meaningful Use Reporting Period
1) If the desired reporting period is not found, it can be entered in the Meaningful Use Measure Reporting Period code table
c. Select a Provider
d. Click Submit
e. The Meaningful Use measures are calculated for the selected Meaningful Use Objective Set, Meaningful Use Reporting Period and Provider. The results are displayed. Click Update to record the results for the EP.
f. Repeat for each EP
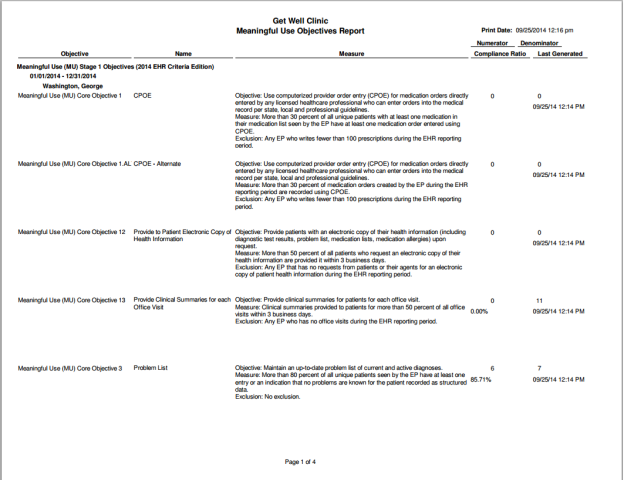
C. Meaningful Use Measure Report for all EPs
1. Administration Reports>Meaningful Use Measure Report
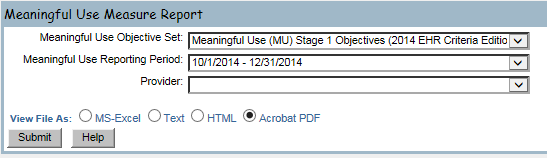
a. Select a Meaningful Use Objective Set
b. Select a Meaningful Use Reporting Period
c. Click Submit
d. The calculated Meaningful Use measures for each EP are displayed in the desired format grouped by Provider. Display format options are: MS-Excel, Text, HTML and Acrobat PDF.
D. DrFirst Meaningful Use Measure Report for each EP.
1. In DrFirst, go to “Additional Options”, under “Reports”, click either “MU Stage 1 Report” or “MU Stage 2 Report”.
2. Select an EP and a date range, then click the “Create Report” button.
3.
The
following Meaningful Use Measures are in DrFirst: CPOE, ePrescribing, Medication List, Allergy
List, and Patient Education (for Medications).
4.
Clinical
Quality Measure Recording
Related Links:
1. eCQM Library (June 2013 Update): http://cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014_EP_MeasuresTable_June2013.pdf
2. CMS’s CQM page: http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeasures.html
NOTE: Epitomax is currently certified on the CQMs defined in the June 2013 EP Update.
CMS165v2: Controlling High Blood PressureMeasure: Percentage of patients 18-85 years of age who had a diagnosis of hypertension and whose blood pressure was adequately controlled (<140/90mmHg) during the measurement period. Initial Patient Population: Patients
18-85 years of age who had a diagnosis of essential hypertension within the
first six months of the measurement period or any time prior to the
measurement period Numerator: Patients whose blood pressure at the most recent visit is adequately controlled (systolic blood pressure < 140 mmHg and diastolic blood pressure < 90 mmHg) during the measurement period. Denominator: Equals Initial Patient Population. Exceptions: None Exclusions: Patients with evidence of end stage renal disease (ESRD), dialysis or renal transplant before or during the measurement period. Also exclude patients with a diagnosis of pregnancy during the measurement period. |
A. Essential hypertension is indicated by an appropriate diagnosis on the Diagnosis tab of the client record.
B. Adequately control blood pressure is determined by blood pressure data on the Vital Stats tab of the client record.
C. End stage renal disease, Dialysis, and renal transplant are indicated by events on the Events tab of the admission. The event type should be set to either Procedure or Intervention, and the treatment should be indicated by an appropriate CPT code or SNOMEDCT Concept on the event.
D. Pregnancy is indicated by an appropriate diagnosis on the Diagnosis tab of the client record.
CMS156v2: Use of High-Risk Medications in the ElderlyMeasure: Percentage of patients 66 years of age and older who were ordered high-risk medications. Two rates are reported. a. Percentage of patients who were ordered at least one high-risk medication. b. Percentage of patients who were ordered at least two different high-risk medications. Initial Patient Population: Patients
66 years and older who had a visit during the measurement period Numerator 1: Patients with an order for at least one high-risk medication during the measurement period. Numerator 2: Patients with an order for at least two different high-risk medications during the measurement period. Denominator: Equals initial patient population. Exceptions: None Exclusions: None |
A. High risk medications for the elderly are entered using DrFirst.
CMS155v2: Weight Assessment and Counseling for Nutrition and Physical Activity for Children and AdolescentsMeasure: Percentage of patients 3-17 years of age who had an outpatient visit with a Primary Care Physician (PCP) or Obstetrician/ Gynecologist (OB/GYN) and who had evidence of the following during the measurement period. Three rates are reported. - Percentage of patients with height, weight, and body mass index (BMI) percentile documentation - Percentage of patients with counseling for nutrition - Percentage of patients with counseling for physical activity Initial Patient Population: Patients
3-17 years of age with at least one outpatient visit with a primary care
physician (PCP) or an obstetrician/ gynecologist (OB/GYN) during the
measurement period Numerator 1: Patients who had a height, weight and body mass index (BMI) percentile recorded during the measurement period Numerator 2: Patients who had counseling for nutrition during the measurement period Numerator 3: Patients who had counseling for physical activity during the measurement period Denominator: Equals initial patient population Exceptions: None Exclusions: None |
A. Height, weight, and body mass index (BMI) are recorded on the Vital Stats tab of the Client Record.
B. Counseling for nutrition is recorded on the Vital Stats tab of the Client Record.
C. Counseling for physical activity is recorded on the Vital Stats tab of the Client Record.
CMS138v2: Preventive Care and Screening: Tobacco Use: Screening and Cessation InterventionMeasure: Percentage of patients aged 18 years and older who were screened for tobacco use one or more times within 24 months AND who received cessation counseling intervention if identified as a tobacco user Initial Patient Population: All patients aged 18 years and older Numerator: Patients who were screened for tobacco use at least once within 24 months AND who received tobacco cessation counseling intervention if identified as a tobacco user Denominator: Equals initial patient population. Exceptions: Documentation of medical reason(s) for not screening for tobacco use (e.g., limited life expectancy, other medical reason) Exclusions: None |
A. Smoking status and tobacco cessation counseling interventions are documented on the Smoking Status tab of the Client Record.
B. Limited life expectancy is indicated with an appropriate diagnosis on the Diagnosis tab of the Client Record.
CMS126v2: Use of Appropriate Medications for AsthmaMeasure: Percentage of patients 5-64 years of age who were identified as having persistent asthma and were appropriately prescribed medication during the measurement period. Initial Patient Population: Patients 5-64 years of age with persistent asthma and a visit during the measurement period Numerator: Patients who were dispensed at least one prescription for a preferred therapy during the measurement period Denominator: Equals initial patient population. Exceptions: None Exclusions: Patients with emphysema, COPD, cystic fibrosis or acute respiratory failure during or prior to the measurement period |
A. Persistent asthma is indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
B. Prescriptions for preferred asthma therapy are entered using DrFirst.
C. Emphysema, COPD, cystic fibrosis, and acute respiratory failure are indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
CMS154v2: Appropriate Treatment for Children with Upper Respiratory Infection (URI)Measure: Percentage of children 3 months-18 years of age who were diagnosed with upper respiratory infection (URI) and were not dispensed an antibiotic prescription on or three days after the episode. Initial Patient Population: Children age 3 months to 18 years who had an outpatient or emergency department (ED) visit with a diagnosis of upper respiratory infection (URI) during the measurement period Numerator: Children without a prescription for antibiotic medication on or 3 days after the outpatient or ED visit for an upper respiratory infection Denominator: Equals initial patient population. Exceptions: None Exclusions: Exclude children who are taking antibiotics in the 30 days prior to the date of the encounter during which the diagnosis was established. Exclude children who had an encounter with a competing diagnosis within three days after the initial diagnosis of URI. |
A. Upper respiratory infection (URI) is indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
B. Prescriptions for antibiotic medications are entered using DrFirst.
C. Competing conditions for respiratory conditions are indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
CMS136v3: ADHD: Follow-Up Care for Children Prescribed Attention-Deficit/Hyperactivity Disorder (ADHD) MedicationMeasure: Percentage of children 6-12 years of age and newly dispensed a medication for attention-deficit/hyperactivity disorder (ADHD) who had appropriate follow-up care. Two Rates are reported: a. Percentage of children who had one follow-up visit with a practitioner with prescribing authority during the 30-Day Initiation Phase. b. Percentage of children who remained on ADHD medication for at least 210 days and who, in addition to the visit in the Initiation Phase, had at least two additional follow-up visits with a practitioner within 270 days (9 months) after the Initiation Phase ended. Initial Patient Population 1: Children 6-12 years of age who were dispensed an ADHD medication during the Intake Period and who had a visit during the measurement period Initial Patient Population 2: Children 6-12 years of age who were dispensed an ADHD medication during the Intake Period and who remained on the medication for at least 210 days out of the 300 days following the IPSD, and who had a visit during the measurement period. Numerator 1: Patients who had at least one face-to-face visit with a practitioner with prescribing authority within 30 days after the IPSD Numerator 2: Patients who had at least one face-to-face visit with a practitioner with prescribing authority during the Initiation Phase, and at least two follow-up visits during the Continuation and Maintenance Phase. One of the two visits during the Continuation and Maintenance Phase may be a telephone visit with a practitioner. Denominator: Equals initial patient population. Exceptions: None Denominator Exclusion 1: Exclude patients diagnosed with narcolepsy at any point in their history or during the measurement period. Exclude patients who had an acute inpatient stay with a principal diagnosis of mental health or substance abuse during the 30 days after the IPSD. Exclude patients who were actively on an ADHD medication in the 120 days prior to the Index Prescription Start Date. Denominator Exclusion 2: Exclude patients diagnosed with narcolepsy at any point in their history or during the measurement period. Exclude patients who had an acute inpatient stay with a principal diagnosis of mental health or substance abuse during the 300 days after the IPSD. Exclude patients who were actively on an ADHD medication in the 120 days prior to the Index Prescription Start Date. |
A. ADHD Medications are entered using DrFirst.
B. Narcolepsy is indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
CMS2v3: Preventive Care and Screening: Screening for Clinical Depression and Follow-Up PlanMeasure: Percentage of patients aged 12 years and older screened for clinical depression on the date of the encounter using an age appropriate standardized depression screening tool AND if positive, a follow-up plan is documented on the date of the positive screen. Initial Patient Population: All patients aged 12 years and older before the beginning of the measurement period with at least one eligible encounter during the measurement period. Numerator: Patients screened for clinical depression on the date of the encounter using an age appropriate standardized tool AND if positive, a follow-up plan is documented on the date of the positive screen Denominator: Equals initial patient population. Exceptions: Patient Reason(s) - Patient refuses to participate OR Medical Reason(s) - Patient is in an urgent or emergent situation where time is of the essence and to delay treatment would jeopardize the patient's health status OR Situations where the patient's functional capacity or motivation to improve may impact the accuracy of results of standardized depression assessment tools. For example: certain court appointed cases or cases of delirium Exclusions: Patients with an active diagnosis for Depression or a diagnosis of Bipolar Disorder |
A. Screening for clinical depression using an age appropriate standardized tool is indicated by an event on the Events tab of the Admission. Use either the “Screen for Clinical Depression: Negative” or “Screen for Clinical Depression: Positive” event type. Use the “Follow-up Plan” field on the event to document the follow-up plan.
B. Depression and bipolar disorder are indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
CMS68v3: Documentation of Current Medications in the Medical RecordMeasure: Percentage of visits for patients aged 18 years and older for which the eligible professional attests to documenting a list of current medications using all immediate resources available on the date of the encounter. This list must include ALL known prescriptions, over-the-counters, herbals, and vitamin/mineral/dietary (nutritional) supplements AND must contain the medications' name, dosage, frequency and route of administration. Initial Patient Population: All visits occurring during the 12 month reporting period for patients aged 18 years and older before the start of the measurement period Numerator: Eligible professional attest to documenting, updating or reviewing the patient's current medications using all immediate resources available on the date of the encounter. This list must include ALL known prescriptions, over-the-counters, herbals and vitamin/mineral/dietary (nutritional) supplements AND must contain the medications' name, dosages, frequency and route of administration. Denominator: Equals initial patient population. Exceptions: Medical Reason: Patient is in an urgent or emergent medical situation where time is of the essence and to delay treatment would jeopardize the patient's health status Exclusions: None |
A. Documenting, updating, or reviewing the patient’s current medications is indicated by an event on the Events tab of the Admission. Use the “Documented/Updated/Reviewed Current Meds” event type.
B. To indicate an exception due to a medical reason, enter an event on the Events tab of the Admission and use the “Documented/Updated/Reviewed Current Meds – NOT Done” event type.
CMS75v2: Children who have Dental Decay or CavitiesMeasure: Percentage of children, age 0-20 years, who have had tooth decay or cavities during the measurement period. Initial Patient Population: Children, age 0-20 years, with a visit during the measurement period. Numerator: Children who had cavities or decayed teeth. Denominator: Equals initial patient population. Exceptions: None Exclusions: None |
A. Cavities and decayed teeth are indicated by an appropriate diagnosis on the Diagnosis tab of the Client Record.
CMS50v2: Closing the referral loop: receipt of specialist reportMeasure: Percentage of patients with referrals, regardless of age, for which the referring provider receives a report from the provider to whom the patient was referred. Initial Patient Population: Number of patients, regardless of age, who were referred by one provider to another provider, and who had a visit during the measurement period. Numerator: Number of patients with a referral, for which the referring provider received a report from the provider to whom the patient was referred. Denominator: Equals initial patient population. Exceptions: None Exclusions: None |
A. A referral is indicated using the Referral History screen within the External Care Givers tab of the admission.
B. Receipt of a report from the referring provider is indicated using an event on the Events tab of the admission. Use the “Receipt of Specialist Report” event type.
Clinical
Quality Measure Reporting
A. Code Tables
1. Added new Meaningful Use Measure Reporting Period code table.
a. Additional reporting periods can be entered in this table, particularly if you are reporting for a 3 month period
b. Reporting periods can be deactivated in this table
c. This same code is used for both Clinical Quality Measure (CQM) and Meaningful Use (MU) Measure Reporting Periods
B. Clinical Quality Measure Calculation for each EP
1. Administration Reports>Clinical Quality Measure Calculation
a. Select a CQM Set
b. Select a CQM Reporting Period
1) If the desired reporting period is not found, it can be entered in the Meaningful Use Measure Reporting Period code table
c. Select a Provider
d. Click Submit
e. The Clinical Quality measures are calculated for the selected CQM Set, CQM Reporting Period and Provider. The results are displayed.
![]()
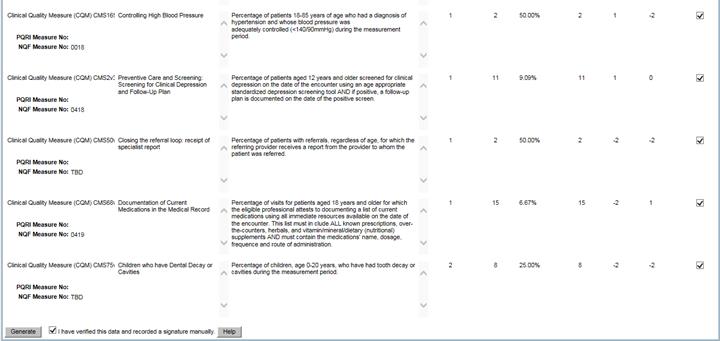
f. Exclude certain Clinical Quality Measures by un-checking the “Include” checkbox on the far right
g. Verify the data for the included measures and record a signature manually on paper outside of Epitomax to indicate that you have done so
h. Check the “I have verified this data and recorded a signature manually.” checkbox at the bottom
i. Click Generate
j.
The
Quality Reporting Document Architecture Calculated Summary Report is displayed
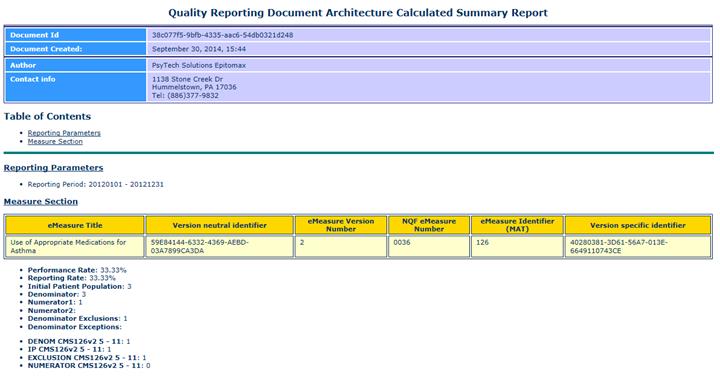
k. The list of CQM measures generated for the EP are displayed. Download the most recently created file.
l. Repeat for each EP